My onset of schizophrenia didn’t occur until long after I’d left home. I was twenty-six years old and just starting college when the hallucinations began. During Fall semester in 1996, I met a fellow student named Holly. She said that our Psychology professor liked me.It wasn’t until I started having dreams of my being murdered that my life with Holly and my professor became more chaotic. It was sometime in November 1996 that the first nightmare occurred. In the dream, I went for my daily walk in Normandale Lake Park. I was on the south side when my Psychology instructor saw me and smiled. I turned away embarrassed and when I looked back he was so close then I saw his face. He was raging mad and lunged at me. I saw my long blonde, curly hair fly in front of my face. Then I felt his hands struggling with me and then he was on top of me. I didn’t have time to scream in my dream; however, I always woke screaming.
Holly didn’t like me talking about my dreams. It disturbed her because she thought that it couldn’t be me since I never had long blonde hair. Instead, the thought it was an older female that I knew back in high school. Holly thought that maybe I subconsciously wanted that former acquaintance dead but she was wrong. I didn’t. I swear. As the dream progressed, I realized that it wasn’t me in the dream but Holly. That is when she started getting more upset about me talking about my dreams, so I stopped sharing them with her.
Anyway, our college lives became anxiety-ridden, especially since our Psychology teacher started following us around. He was also faculty advisor so he was friends with everyone, meaning he was everywhere: in and out of our other classrooms. Then the maintenance men started watching us, too, particularly me. It didn’t matter where I sat (lunchroom, out front, in the Japanese garden, on hallway floors, in the library or computer center), our Psych professor would find me.
The dreams went on for months when one day I was watching television while doing dishes. At that moment, my body froze. I saw her—the blonde with long hair that was being murdered in my dream—and knew immediately who it was. It was my friend, Holly! The news report said that a pedophile had killed her in Normandale Lake Park. It couldn’t be right.
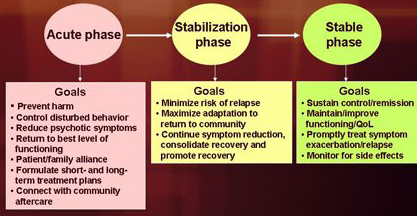
During my psychotic break, I was hallucinating visions and voices as well as deep in delusion. I was seeing a dead woman in my house as well as my deceased grandma and aunt. In addition, I thought I could walk through as well as see and hear through walls to my adjacent neighbors townhouse. Plus, I was deep in paranoia in thinking someone was following me wherever I went.
My psychotic break or nervous breakdown occurred over a six month period. Initially there were confusing voices and overwhelming smells but that progressed into debilitating paranoia, delusion, and non-stop hallucinations. I refused medication because I thought it would cloud my thought processes which were relaying danger, danger, danger…. I was worried that my family and I wouldn’t be safe if I took the medication. I thought the dead woman that lives inside our home would cause us harm. Plus I was concerned that it (meds) would control my thoughts and take over our wellbeing so that we couldn’t deal with the watchers. In reality, it was all unreal. In the emergency room, I was forced to take Seroquel which knocked me out. It was in the moments upon awakening that I realized all the voices, visions, smells, and sounds STOPPED. It was quiet for the first time in a long while. Fortunately, for me, family members made certain that I stayed on the medication regimen. Yes, it has gone through changes where I’ve had to switch meds but all in all the majority of the hallucinations and delusions have stayed away. Stressors still bring on bouts but for the most part the drug therapy helps. At first, I kept in mind that I could always stop the meds and bring back the positive hallucinations; but now I know the bad will come along with the good. While I miss the visions of my deceased grandma and aunt, I don’t miss the bad spirits.
I’m also an enrolled member of the Sisseton-Wahpeton Oyate. Thanks in part to fantastic foster parents, sassy social workers, and outstanding teachers, I’m also a family-focused parent of four wonderful young adults. I’ve self-published one memoir under my own name and four fiction novels under a pseudonym, Peyton Mathie. Those accounts were based on my life stories. Although I’m a native of the Lake Traverse reservation in South Dakota, I lived in Brooklyn, New York off and on throughout my childhood. Currently, I reside in Eden Prairie, Minnesota with my family. My hobbies include yoga, MBSR, camping, budget travel, and painting.
Note: The pseudonym was derived from the first name of my daughter’s childhood friend and the surname of a coworker at approximately the same time frame. In one I saw signs of my past and the latter, hopefully, my future.
Like this:
Like Loading...















You must be logged in to post a comment.